Beyond Vacancy™ · Season 1 · Workforce Architecture 03 Published by Shalini Sood | beyondvacancy.co.in
Workforce Architecture 03 – Why Workforce Pipelines Collapse Even When Talent Exists

The pipeline was full.
Forty nurses. Verified qualifications. Valid passports. Signed offer letters. A European hospital partner is waiting. Months of preparation on every side.
And then the hospital re-advertised.
I have seen this more times than I can count in eleven years of building international healthcare workforce pathways. And every single time, the instinct from the hospital side is the same: blame the candidates. Blame the sending country. Blame the market.
Rarely: examine the pipeline itself.
Because the pipeline looked fine. It was full. The talent existed. The numbers were there.
What was not there — what almost nobody builds deliberately — was governance.
A Pipeline Is Not a List
The word “pipeline” has become so common in healthcare recruitment that it has almost lost its meaning. Every agency has a pipeline. Every HR director asks about the pipeline. Every board presentation includes a pipeline slide.
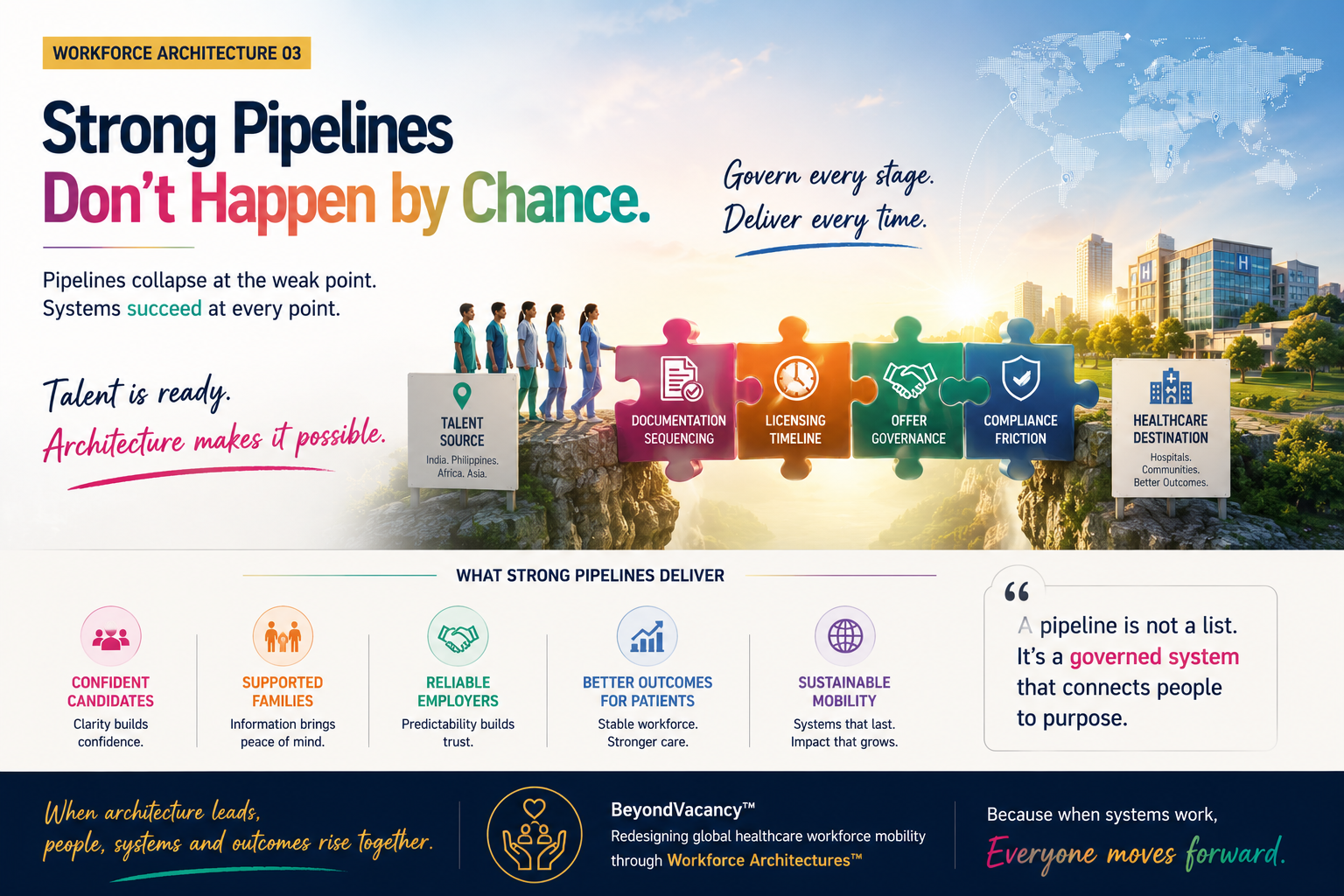
A list of candidates is not a pipeline. A pipeline, in the true engineering sense of the word, is a sequenced, governed, compliance-validated system with active management at every stage.
When engineers design a physical pipeline — for water, for gas, for oil — they do not simply connect a source to a destination and assume the flow will happen. They design pressure regulators, monitoring systems, failsafes, and maintenance protocols for every kilometer of the route. A pipeline without governance is not a pipeline. It is a series of disconnected segments that happen to be pointing in the same direction.
International healthcare workforce pipelines work identically.
The source exists in India, the Philippines, Nigeria, Kenya, and South Asia. Qualified, internationally mobile healthcare professionals in genuine numbers. The destination exists — European healthcare systems, GCC hospitals, Australian aged care facilities, Japanese clinical networks — with real, documented, urgent need.
What consistently collapses is the architecture between them.
The Four Points Where Pipelines Fail
In eleven years of operational experience, I have identified four specific layers where healthcare workforce pipelines collapse. Not occasionally. Routinely. And the collapse at any single layer is enough to bring the entire pipeline down.
Layer One — Documentation Sequencing
International healthcare deployment requires a precise sequence of documents — not just the right documents, but the right documents obtained in the right order, from the right authorities, within validity windows that differ by destination country.
A qualification certificate notarized before an equivalency assessment is submitted. A language certification obtained before an eligibility determination. A police clearance obtained twelve months before deployment, when the receiving country requires it within six months of arrival.
Each of these errors costs weeks. Sometimes months. In a process that is already twelve to eighteen months long, a sequencing error at month four can compress an entire candidate cohort into a single delay point — and when candidates hit a wall simultaneously, confidence collapses.
We had a cohort of fourteen nurses preparing for deployment to a GCC hospital. Eleven of them had submitted language certifications before their professional registration equivalency had been formally acknowledged by the receiving country’s health authority. Three weeks before the processing deadline, we discovered the certifications would need to be reissued. Not because the candidates had failed. Because the sequence was wrong.
Eleven candidates resubmitted. Six were completed in time. Five were deferred to the next intake cycle.
A sequencing error. Not a talent shortage.
Layer Two — Licensing Timeline Mismanagement
Every destination country has its own professional licensing authority with its own processing timelines. Some are predictable. Many are not. A licensing application submitted without a buffer for processing delays is a deployment risk that most organizations do not price into their timelines.
When licensing timelines extend — as they regularly do — the cascading effect is immediate. Visa applications cannot be submitted without licensing confirmation. Accommodation cannot be confirmed without a visa date. The candidate, now in a holding pattern with no clear timeline, begins to lose confidence. Their family, watching them put their lives on pause, begins to apply pressure.
Most pipeline managers respond to licensing delays by waiting. The correct response is to activate a parallel communication protocol — regular, specific, honest updates to the candidate about exactly where the application stands, what the expected timeline is, and what the next milestone will be. Silence during a licensing delay is not neutral. It is corrosive.
Layer Three — Offer Governance Breakdown
An offer letter is not the end of a process. It is the beginning of the most fragile phase of the entire deployment.
Between offer and arrival, a candidate is simultaneously managing a professional transition, a personal life transition, a family system change, and a financial commitment — all without yet having the security of being at their destination. The offer exists on paper. The reality does not yet exist in their lives.
During this period, which typically spans six to twelve months in international healthcare deployment, the organization that made the offer has a governance responsibility it rarely exercises. Who is actively maintaining the candidate relationship? Who is checking in monthly — not to chase paperwork, but to understand how the candidate is doing? Who knows when the candidate’s spouse has raised doubts? Who knows when a counteroffer has arrived from a domestic employer?
In the cohort of forty I mentioned at the opening of this piece, offer governance was the primary failure. After signed letters were in place, the hospital HR team assumed the pipeline was secure and moved their attention to the next hiring cycle. The advisory managing the process had no structured check-in protocol for the post-offer period.
By month five, eleven candidates had quietly accepted other positions. By month eight, nine more had deferred citing family circumstances. By the time deployment was scheduled, twenty of the forty had exited. Silently. Without a single formal withdrawal.
The hospital re-advertised. Called it a pipeline failure.
It was a governance failure.
Layer Four — Compliance Validation Gaps
The final layer — and the one that collapses pipelines closest to the finish line, which makes it the most expensive — is compliance validation.
Every destination country has specific compliance requirements that must be met before a candidate can be deployed. Criminal background clearances, health screenings, credential verifications, and insurance registrations. These are not formalities. They are legal requirements that the receiving institution is accountable for.
When compliance validation is treated as a checklist item to be completed in the final weeks before deployment, rather than as an ongoing process managed throughout the pipeline, errors surface at the worst possible moment. A clearance with an unexpected complication. A health screening with a timeline that conflicts with the deployment date. A credential that requires additional verification from a university that takes six weeks to respond.
At that stage, the hospital has rostered the candidate. The candidate has given notice. The family has decided. And the pipeline collapses at the final gate.
What This Costs the People Inside the Pipeline
Twenty of the forty candidates exited quietly. No formal withdrawal. No single dramatic failure point. Just a slow erosion of confidence across six to eight months of silence.
Each of those twenty had a family who had begun preparing for their absence. Some had already discussed which grandparent would help with the children. Some had given notice at jobs that paid less but were certain, in exchange for a future that was supposed to be more certain still.
The hospital experienced this as a recruitment delay. The twenty candidates experienced it as a life decision that collapsed without ever being told why.
This is the part of the pipeline failure that does not appear in any HR dashboard. It does not reduce to a percentage. It is the precise human cost of treating a workforce pipeline as a numbers exercise rather than a governed system responsible for the people moving through it.
The Distinction Between Building and Governing
Most organizations that manage international healthcare hiring understand pipeline building. They know how to identify candidates, screen qualifications, conduct interviews, and issue offers.
Very few understand pipeline governance.
Building a pipeline means assembling candidates. Governing a pipeline means actively managing every layer, at every stage, with defined ownership, defined escalation protocols, and defined candidate communication standards — treating the pipeline not as a static list but as a living system that requires constant monitoring and intervention.
The joining ratio — the percentage of candidates who successfully complete the journey from offer to arrival and deployment — is the single most honest metric of pipeline health. In organizations without pipeline governance, joining ratios typically sit between twenty and forty percent. In organizations with structured governance frameworks, joining ratios consistently reach seventy to eighty-five percent.
That gap is not a talent market difference. It is a governance difference.
At, The Indah People, the Pipeline Governance Framework we have developed over eleven years addresses all four failure layers with specific protocols: document sequencing maps for every destination country, licensing timeline buffers built into every project plan, monthly candidate relationship management during the post-offer period, and rolling compliance validation integrated throughout the process rather than concentrated at the end.
The pipeline does not collapse because the talent does not exist.
It collapses because the system that should carry that talent was never properly designed, monitored, or governed.
What Your Pipeline Is Actually Telling You
If your joining ratio is below sixty percent, your pipeline has a governance problem.
If your pipeline regularly looks full and still produces insufficient deployments, your pipeline has a sequencing problem.
If you are regularly re-advertising positions you filled twelve months ago, your pipeline has an offer governance problem.
These are not separate crises. They are symptoms of the same root failure, diagnosable and fixable — but only with a fundamentally different approach than the one that created them.
You cannot govern a pipeline you have not designed. You cannot monitor a system you have not mapped. And you cannot fix a governance failure by adding more candidates to the top of a broken process.
The talent exists. It has always existed.
If your organisation’s joining ratio is below sixty percent, which of the four layers — documentation sequencing, licensing timelines, offer governance, or compliance validation — do you suspect is failing first?
Share your perspective in the comments.
Shalini Sood is the Founder of The Indah People and a Global Healthcare Mobility Architect with 11 years of experience designing cross-border workforce systems across Europe, the GCC, Japan, Australia, and New Zealand. She writes about workforce architecture, career mobility, and the future of global healthcare talent at beyondvacancy.co.in.
For workforce advisory enquiries: theindahpeople.in
Beyond Vacancy™ is a knowledge platform on global healthcare workforce mobility.
Season 1 — Designing Global Healthcare Mobility
Next: Workforce Architecture 04 — The Hidden Cost of Delayed Deployment

Leave a comment